The COVID-19 pandemic has shone the spotlight on the state of world health and how we must prepare ourselves in the near future for the spread of hitherto unknown viruses. Hospitals undoubtedly play an important role in managing the health of everyone, and they must innovate to improve their response to new challenges, one of which is the ageing of the global population.
The research by Design & Health Lab of the Department of Architecture, Building Engineering and the Built Environment (DABC) at the Politecnico di Milano focuses precisely on these issues, successfully developing indicators and guidelines that have also been adopted in a document by the World Health Organisation. We talk to researcher Andrea Brambilla, who has been interested in hospital architecture since his master’s thesis with a project at the Alta Scuola Politecnica led by Professor Stefano Capolongo, going on to continue his research at the Politecnico.
“After graduating, I was a consultant for a project by Fondazione Politecnico and EY on hospital organisation, and at the same time I was doing a master’s in hospital design,” says the researcher. “I had the opportunity to visit hospitals in Lombardy and assess their organisational performance, their medical records, aspects that apparently had nothing to do with architecture. Every day, I wondered why, among all the performance evaluation parameters of the facilities, there was not one related to the space occupied by the patients and staff.
Perhaps this was the moment when I thought of doing my PhD on the subject of evaluating hospital architecture. For the first time, we reflected on what were the measurable elements of architecture in order to achieve a better, more pleasant, more efficient, more sustainable, more digital hospital.
During my doctoral studies at the Politecnico di Milano and Chalmers University of Technology in Sweden, thanks to an IDEA League research grant, I had the opportunity to experience a situation at the forefront in this area, with a multidisciplinary approach. The first researcher of these topics, Roger Ulrich, taught at Chalmers. He is a doctor (not an architect) who conducted an experiment in the 1980s, dividing a group of patients into two subgroups: the first was in a room where the window looked out onto other buildings, the second had a view of a green area. It turned out that, all things being equal, patients in the second group had a much faster recovery time, involving less medication and less stress. This study is the basis for research in Evidence-Based Design, the design of architectures for health based on scientific and measurable evidence.
Andrea Brambilla
The goal of a hospital is to improve patient care: the physical space can also help in this sense.
Andrea Brambilla
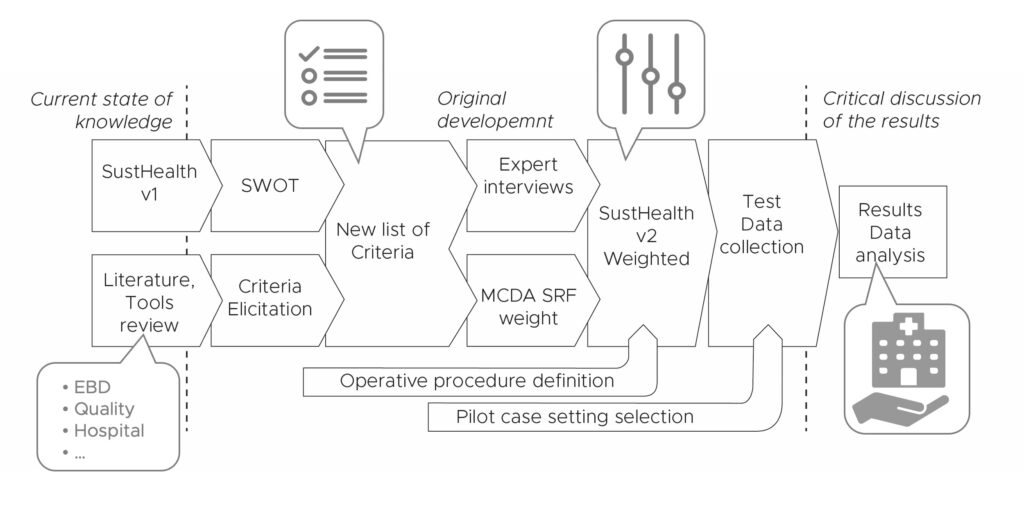
My research topic is the evaluation of the architecture and sustainability of hospitals, not only in environmental terms but also from a social and organisational perspective. I started with an existing performance mapping tool, developed by the research group where I work at the Politecnico, and implemented it in terms of the sustainability of a hospital organisation. I ‘calibrated’ it with experts in multi-criteria analysis methodology and tested it on a few cases to see how it worked. This tool can provide the General Manager with a holistic and objective view on the sustainability of the facility and where to invest to improve performance: an approach that is regularly used in healthcare to choose equipment or personnel. The tool forms the basis of a spin-off we are launching, thanks to a business partner.
The goal of a hospital is to improve patient care: the physical space can also help in this sense.
Your PhD coincided with the SARS COVID-19 pandemic – a period of great stress for hospitals. What lessons did you learn in the field?
«At that time, hospitals were changing day by day: I understood the importance of the concept of flexibility applied to hospitals and research.
Hospitals change not only with pandemics, but like all ‘social architectures’, due to the slower and less palpable changes in society. Just think that with an ageing population they will be a place predominantly inhabited by the elderly or dealing with the issue of climate change. The architecture and design must change accordingly: this is the most important lesson I have learnt.
Hospital space is important not only in terms of organisation, but also in terms of infection-related issues. Indeed, the risk of contracting the notorious care-related infections must be mitigated».
Methodological process for the development of the evaluation tool
The pandemic also shone the light on the issue of community healthcare. What did you deduce from your research on this topic?
«Within the research group, we were also responsible for drafting guidelines for
Agenas – the National Agency for Regional Health Services – on the design of community houses, community hospitals and regional control centres. Some regions before the pandemic were further ahead than others with a different focus on the local community.
In other countries, lower-intensity facilities were already being developed to deliver ‘low-care’ services adapted to the social contexts and socio-demographic and epidemiological characteristics of the local area. The hospital is not a single organism, but part of a system».
Cover of the Technical Brief written for the World Health Organization by the Design & Health Lab (POLIMI authors S. Capolongo, A. Brambilla, , M.Gola)
The World Health Organisation presented in Baku (Azerbaijan) the new design recommendations for new hospitals to be built in the European Region, the result of a research partnership with the Politecnico di Milano. The document ‘Hospitals of the Future’ was produced by your laboratory and you are among the authors. How did you develop it? Have you added anything more to previous research?
«The work is the result of the monitoring initiated during COVID-19. As a department, we ran the ‘observatory’ on Resilient Hospitals and I was in the research group that drew up a decalogue of strategies for ‘post-COVID’ hospitals. The WHO asked us to go one step further: to really look into the future – not just post-pandemic – and put down on paper for the European Region how hospital needs have changed, which was a big challenge for us.
The recommendations have been divided into macro-areas: on the one hand, we look at the hospital in relation to the outside, to the context, so the issues of location, relations with the local area, with the local health network, green spaces, accessibility, transport.
The second chapter instead looks inside the hospital, at the features it must have: from flexibility to the possibility of managing risks and infections, to user comfort. We focused a lot on the topic of single rooms, sustainability and security because these were somewhat the key issues also at the European policy level, especially for those states not yet members of the EU but geographically related. The last part emphasises precisely the issues of the measurability of guidelines, suggesting tools to help designers manage the process and not just the project as a set of keywords.
The technical brief has been read and adopted by many entities at the European level and many have started to ask for support to implement it. The first experience was in Moldova, where due to a problem of proximity and border with Ukraine, there is also an issue of war-related health migration.
We have helped institutions to apply these strategies in a real context, so much so that we have started a process of accreditation as a ‘collaborating centre’ for the WHO: among the accredited research centres, the Politecnico di Milano will be the first technical-scientific institution in the world.
Measurability also comes into play in the Joint Research Partnership ‘Healthcare Infrastructures’ (JRP HI) of which the ABC Department is a promoter together with the Fondazione Politecnico, a national research platform with a large network of companies and institutions, to outline truly measurable requirements for hospitals.
This second experience is more related to our [the Italian] health system (which has its own characteristics, its own limitations, including regulatory ones): being highly regulated, innovation has be be achieved in compliance with certain general rules, which is a difficult but stimulating challenge».
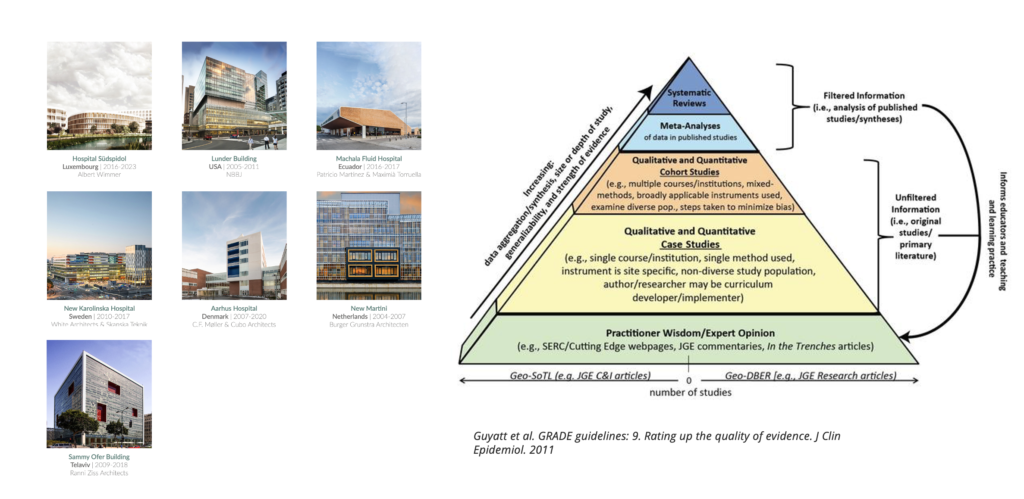
Evidence and Practice-based approach: the research results are based on scientific evidence and international case studies analyses
To date, there is no up-to-date national (or European) performance standard for hospital buildings. UNI – the Italian National Agency for Standardisation – recently set up a Working Group coordinated by Prof. Stefano Capolongo to draft a Technical Standard on hospital design, in which you are involved. How did this project come about?
Before issuing a standard, a terminology standard is developed, outlining common definitions to be used. The hospital is such a complex infrastructure with the interaction of different professions that each institution has its own vocabulary. Forexample, the idea of ‘ward’ or ‘department’ is highly dependent on the organisational model: designing a new hospital on the basis of current wards and their beds for some is standard, while for others it is obsolete.
Another example is specific terminology such as flexibility or ‘buffer space’ [TN: in Italian called spazio polmone, literally ‘lung space’ or ‘breathing space’]: in the planner’s common lexicon, this is space that allows for future expansion but is often confused [in Italian] with green space or space for medical gases. Since as early as my PhD, this discrepancy has been glaring».
What are the projects for the future? Are there areas of research you would like to develop?
«Certainly after the COVID experience, I am interested in the topic of care-related infections because it has a great clinical impact on people. We have also submitted project proposals on this at European level. So far, the most solid research on the subject of infections in the physical hospital environment has only been conducted by microbiologists, not architects, because they are familiar with the subject of transmission but do not know the subject of spaces.
I would like to continue working on the topic of measurability by creating mock-ups, models of hospital rooms that can be modified, used, viewed and measured using sensor technology and artificial intelligence systems: simulating how, as the space changes, certain parameters change and certain results are obtained. There are international research centres that are moving in this direction, for example ‘simulation rooms’ are being developed in Switzerland, near Bern.
The third ‘dream’ is to improve the accessibility of data. Today, we do not have a reliable database or mapping of the quality conservation status of our hospital heritage. Without a precise knowledge of the state of affairs, however, it is impossible to research and implement realistic and high-impact solutions for the entire national health system, especially for such a complex and constantly changing infrastructure».
Questo sito utilizza cookie funzionali e script esterni per migliorare la tua esperienza.
Privacy settings
Impostazioni privacy
Questo sito utilizza cookie funzionali e script esterni per migliorare la tua esperienza. A sinistra vengono specificati quali cookie e script sono utilizzati e come influiscono sulla tua visita. È possibile modificare il tuo consenso in qualsiasi momento. Le tue scelte non influiranno sulla navigazione del sito.
NOTE: These settings will only apply to the browser and device you are currently using.
Google Analytics
Google Analytics 4 (GA4) è uno strumento di analisi web fornito da Google che aiuta a monitorare e analizzare il comportamento degli utenti sul sito. Utilizza dati anonimi per raccogliere informazioni sulle interazioni degli utenti, migliorare l’esperienza di navigazione e ottimizzare le prestazioni del sito. GA4 utilizza un modello basato sugli eventi per una misurazione più accurata e offre integrazione con Google Ads e altri strumenti di marketing. I dati vengono raccolti solo con il consenso dell’utente, in conformità con il GDPR e altre normative sulla privacy.
Web Analytics Italia
Web Analytics Italia è una piattaforma nazionale che consente alle amministrazioni di raccogliere e analizzare i dati statistici sul traffico dei propri siti e servizi digitali. Il sistema di raccolta e analisi dei dati web basata sul software Matomo